How is HLH treated?
Firstly the aim for treatment is to reduce the severe excessive inflammation that is responsible for the life-threatening symptoms.
Secondly, treatment aims to kill any of the immune cells that have been infected by a trigger, for example viruses and bacteria. This aims to remove the trigger for the excessive inflammation.
Unfortunately, even if the original infection that triggered the HLH is killed, that is not enough to stop the excessive inflammation, since it has spiralled out of control.
Thirdly, the ultimate aim for children with a genetic cause of HLH is stem cell transplantation. This aims to replace the defective cells in the bone marrow, with healthy cells from a donor.
Treatment is tailored for individual patients, and is guided by the type of HLH your child has, the severity of the severity of the symptoms, the age of the patient, and any other underlying conditions
As HLH is uncommon and serious, treatment is usually coordinated by a specialist centre experienced in treating rare immune disorders.
The priority of treatment is to damp down (suppress) the immune system to reduce the over-reaction and lessen the risk of tissue damage. This will often involve courses of corticosteroids and chemotherapy medicines, usually given into a vein (intravenously) in hospital. Some of the medicines used are listed in the table below but new treatments are being developed all the time. Treatment will be individualized to minimise side effects, which your medical team will discuss with you. If an infectious trigger is suspected, anti-infection treatment may be given, such as antibiotics or other medication.
Type of drug: Example: How it is given
Steroid: Dexamethasone, prednisolone: Daily injection into a vein or by mouth
Calcineurin inhibitor: Cyclosporin: Twice daily, into a vein or by mouth
Cytotoxic chemotherapy: Etoposide: Into a vein, twice weekly at first then less often over time
Methotrexate: By injection into the fluid around the spinal cord, up to four doses weekly if the brain is affected
Biologics: Alemtuzumab: Into a vein, daily for a few days
In the case of primary HLH, this treatment usually puts the condition into remission, but the risk of relapse remains.
Corrective treatment of HLH
In many cases, haematopoietic stem cell transplant (HSCT, including bone marrow transplant, or BMT) offers the potential for long-term cure of primary HLH. HSCT aims to replace the faulty immune system with an immune system from a healthy donor. Stem cells, from which all the cells of the immune system develop, can be obtained from healthy bone marrow, or in some cases from umbilical cord blood or donor blood. The healthy stem cells can be given by transfusion into a vein to a child with HLH.
he symptoms, the age of the patient, and any other underlying conditions.
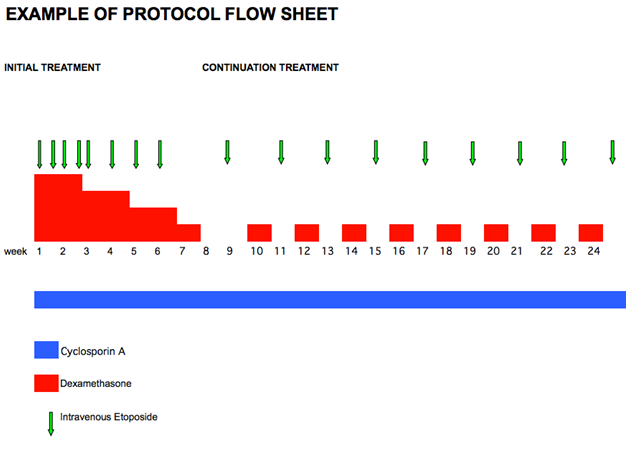
HLH Treatment Protocol
The vast majority of children with HLH will be treated with chemotherapy and immunotherapy guided by an international protocol (see example below), which maps out the dates for the different medications. The protocol will be tailored to your child.
If your child needs chemotherapy, he or she will probably need a central line. This is a tube that is inserted into a large blood vessel and tunnelled under the skin to where it can be easily accessed. It allows blood samples to be taken and treatment, including chemotherapy, to be given easily and painlessly. The central line is put in under general anaesthesia and will stay in place until the end of your child’s treatment. Your hospital will provide more information about the types of central lines they offer.
If your child is unwell or requires more intensive treatment he or she will need to be in hospital. Some children however receive some of their intravenous treatment by visiting their hospital out-patient or day-care facility. This may only be available at your treating oncologist/haematologist’s hospital or at your local hospital under a shared care arrangement with a local doctor. Some treatment, like that taken by mouth, can be given at home.
While on chemotherapy, for up to 6 months afterwards, and up to a year after a bone marrow transplant, your child will be susceptible to infections. This is known as being immunocompromised. If he or she develops a fever or becomes unwell you need to contact your treating team immediately for advice. Your child may need immediate hospital admission and treatment with antibiotics.